Product Tour
Inside the clinician dashboard
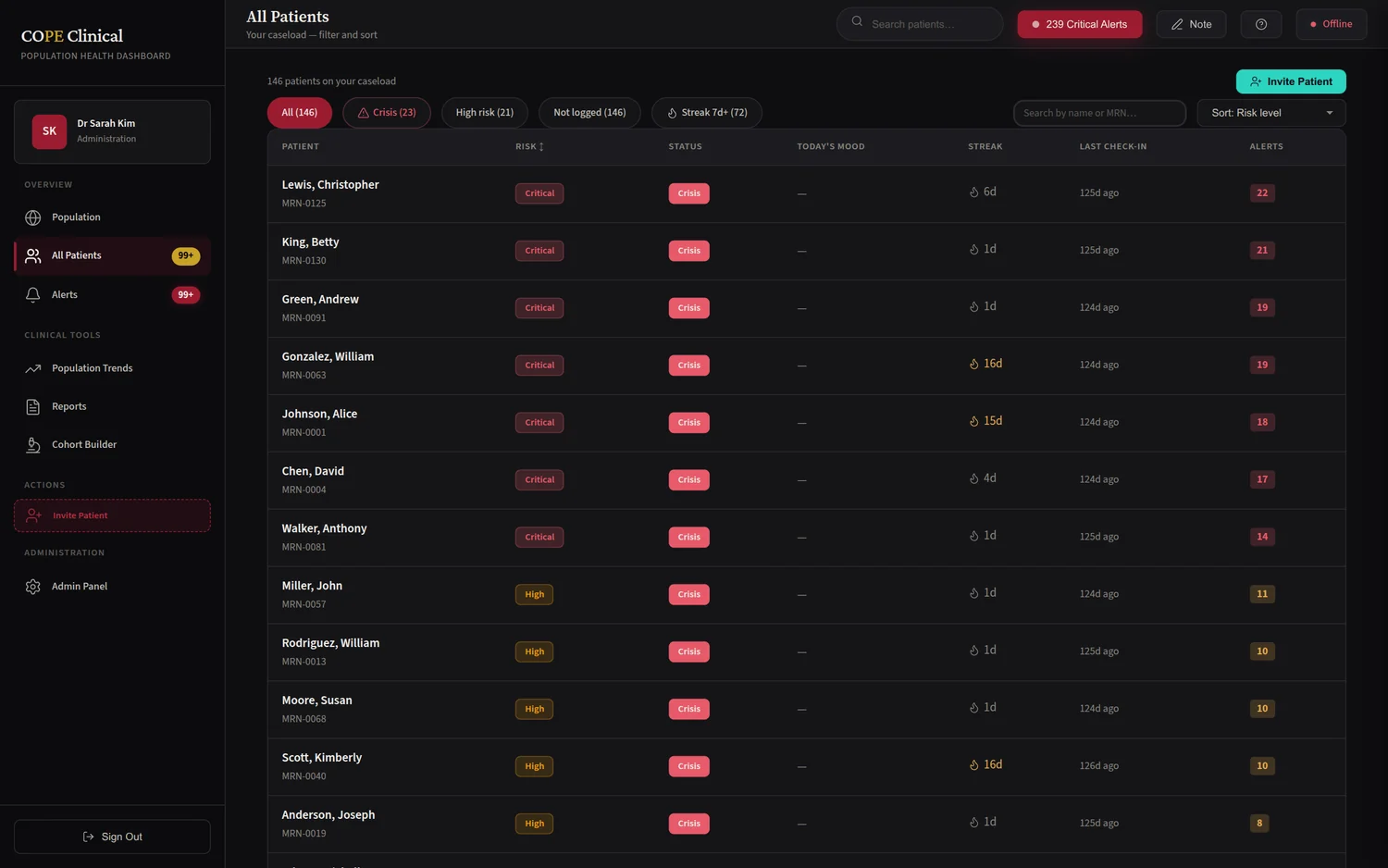
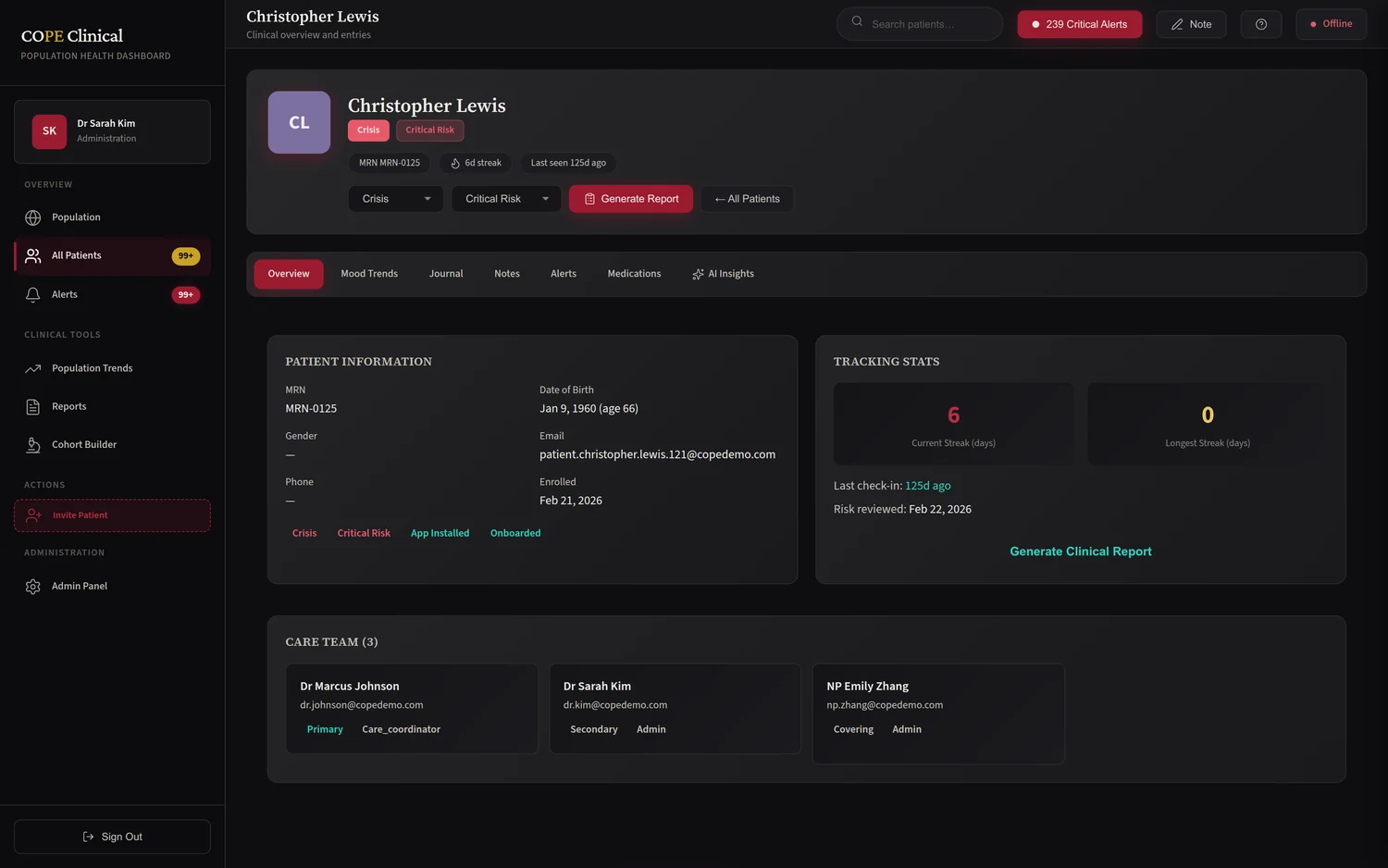
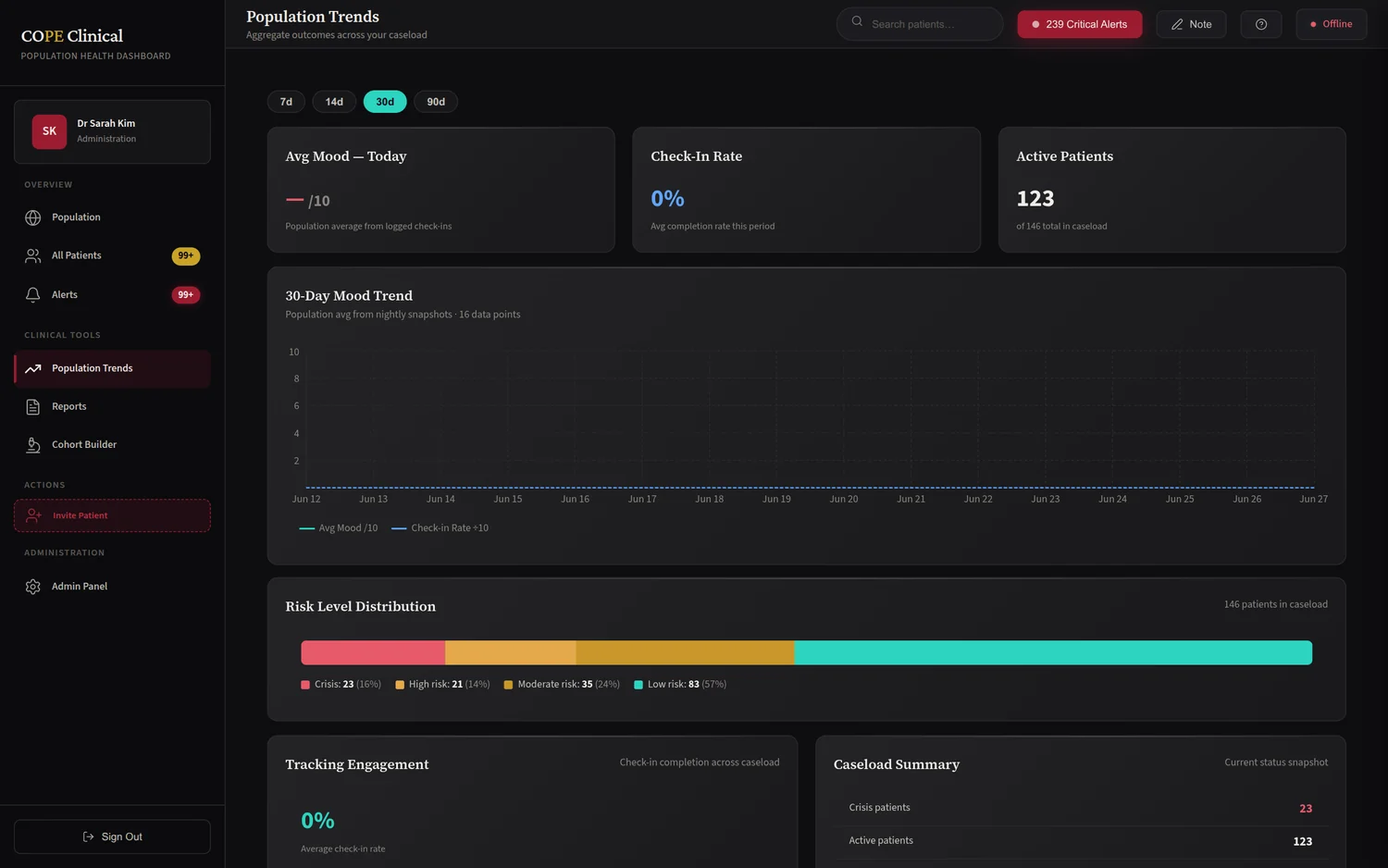
From the live clinician demo on synthetic patients — click any view to enlarge.
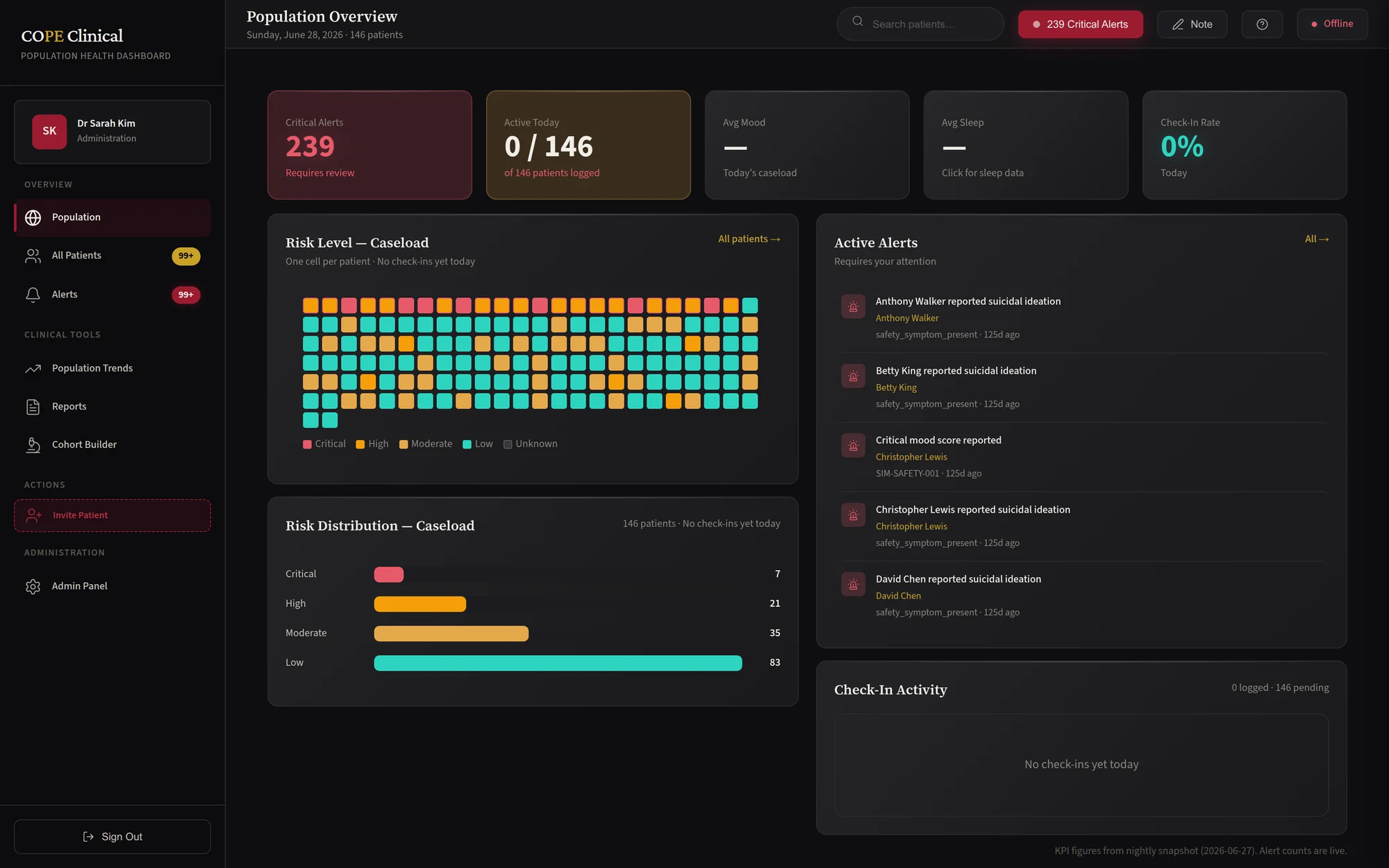
Real-time behavioral health monitoring for clinicians and patients.
COPE re-centers measurement-based care around the clinician. Patients use a native mobile app to log daily mood, sleep, exercise, medication adherence, and symptoms; clinicians monitor cohorts, receive real-time alerts when patients cross clinical thresholds, and generate reports through a web dashboard built around validated psychiatric instruments. FHIR R4 export, first-party authentication, and built-in crisis resources throughout.
The Problem
Behavioral health runs on a crisis-to-appointment cycle: a clinician sees a patient for 30–50 minutes every one to four weeks, then loses visibility until the next visit. A mood can plummet, a side effect can emerge, or suicidal ideation can develop — all invisible until the next appointment. Retrospective recall degrades within days, so clinicians lean on memory and hunches.
Measurement-based care — systematic daily tracking plus validated assessments — is the evidence-based antidote. COPE makes it frictionless for the patient and clinically actionable for the care team, in real time.
Capabilities
A two-to-five minute daily check-in captures mood (1–10), sleep, exercise, and coping — progressively revealing optional clinical domains (mania, anxiety, anhedonia, ideation) based on diagnosis and clinician configuration.
Full response capture for PHQ-9, GAD-7, ISI, C-SSRS, ASRM, and WHODAS 2.0 — LOINC-mapped and FHIR-exportable, with configurable completion windows and automatic threshold alerts.
C-SSRS endorsement of intent triggers a critical alert for immediate clinical review, with inline links to the 988 Suicide & Crisis Lifeline and Crisis Text Line. Patient-authored safety plans capture warning signs, coping strategies, and contacts.
Patients log doses against a clinician-managed medication list; the dashboard surfaces adherence rates to flag non-adherence, with optional notes for side effects and barriers.
Open-ended reflections, optionally shared with the care team, rendered as sanitized markdown — with edit windows that preserve integrity after a clinician has reviewed.
Threshold rules (assessment scores, sharp mood drops, missed medications, ideation) publish over Redis to a clinician WebSocket feed — acknowledge, resolve, or escalate, with full alert history.
Population KPIs and per-panel trends — average mood, alert velocity, adherence — with drill-down to individual patient timelines and assessment score history.
Patient data maps to FHIR resources — Observation, MedicationRequest, Condition, CarePlan, Consent, and QuestionnaireResponse — with a published CapabilityStatement for EHR integration.
Generate formatted PDF summaries — mood graphs, recent assessments, medications, shared journals, and alert history — for the chart or a patient handoff.
Product Tour
From the live clinician demo on synthetic patients — click any view to enlarge.
Architecture
A React Native patient app (iOS + Android) with biometric unlock and a dark, low-friction check-in UI.
A Vite-built clinician dashboard with mandatory TOTP MFA, real-time alerts, and Recharts visualizations.
A typed API across auth, daily entries, assessments, alerts, medications, FHIR, and more — Zod-validated with rate limiting.
Row-level security enforces care-team relationships — clinicians see only their patients — with a HIPAA-style audit trail.
Alert rules publish to Redis and fan out to connected clinicians; BullMQ runs the rules engine and report generation.
bcrypt + TOTP with rotating refresh tokens — no third-party identity vendor (Supabase was retired).
Who It's For
A psychiatrist reviews the dashboard in a few minutes of admin time, spots an ASRM score crossing the hypomania threshold over the weekend, calls the patient, and adjusts the regimen — never missing a destabilization between visits.
Care coordinators track mood stability and adherence across a panel of serious-mental-illness patients, escalating high-risk alerts to supervising psychiatrists, with FHIR export into the center's EHR.
Between appointments, patients log daily mood; at visit time the clinician sees the last 30 days at a glance, and a PDF summary routes to the patient's PCP afterward.
A safety plan authored on the unit is shared with the outpatient team at discharge; real-time alerts flag any mood drop in the first two weeks — the highest-risk window.
Under the Hood
FAQ
Explore the live demo, or talk to us about measurement-based care for your practice.